&geometry(278x56) "Veterinary Specialist Services Pty Ltd.")
Laryngeal Paralysis in Dogs
Laryngeal paralysis is a frequently encountered respiratory condition in dogs characterised by partial to complete failure of abduction of one or both arytenoid cartilages during inspiration resulting in mechanical upper airway obstruction. The intrinsic laryngeal muscles control the abductory and adductory movements of the arytenoid cartilages and vocal folds, subsequently controling the size of the rima glottidis. These intrinsic muscles of the larynx comprise of the cricothyroideus, cricoarytenoideus dorsalis, cricoarytenoideus lateralis, arytenoideus transversus and the thyroarytenoideus. All motor innervation to the intrinsic laryngeal muscles is supplied by the cranial and caudal laryngeal nerves, which arise from the vagus nerve. The caudal laryngeal nerve terminates as the recurrent laryngeal nerve which provides motor innervation to all intrinsic laryngeal muscles, both abductory and adductory, except for the cricothyroideus muscle which receives innervation from the external branch of the cranial laryngeal nerve. The cricoarytenoideus dorsalis muscle is the primary abductor of the arytenoid cartilages and vocal folds.
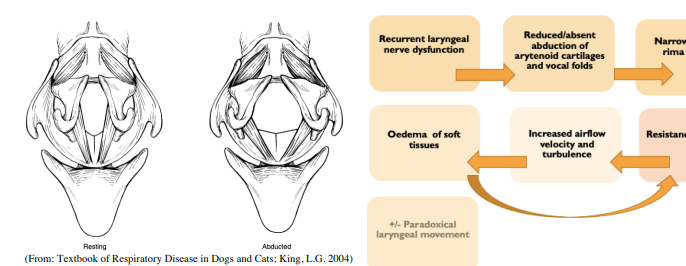
Damage to the supplying recurrent laryngeal nerve results in reduced or absent abduction of the arytenoids and vocal folds during inspiration, narrowing the rima glottidis. This narrowing increases airflow velocity and creates turbulence leading to oedema of the soft tissues, further increasing airflow resistance and turbulence. Paradoxical movement of the arytenoids may occur where they are drawn medially on inspiration, further contributing to airway obstruction. Laryngeal paralysis may be congenital or acquired. The congenital form is uncommon and is seen in young dogs (usually <1y). It has been reported in Bouvier des Flandres, Huskies, Dalmatians, Rottweilers and Bull Terriers. The mechanisms for paralysis and genetic transmission is not known in all breeds.
Acquired laryngeal paralysis is far more common than the congenital form accounting for over 80% of cases. Reported causes of acquired laryngeal paralysis include trauma to the vagus or recurrent laryngeal nerve, organophosphatephate and lead toxicity, hypothyroidism, polyradiculoneuritis and other polyneuropathies. Most commonly no underlying cause is present, and the condition is deemed idiopathic. Idiopathic laryngeal paralysis is most common in middle-aged to older large breed dogs. Labradors, Golden Retrievers, Saint Bernards and Irish Setters are over-represented and males are more commonly affected than females by 2-3 times. Clinical signs: These include altered bark, gagging, coughing, gradual exercise intolerance and characteristic inspiratory stridor, often worse with heat and exercise. Severely affected patients may have episodes of dyspnoea and cyanosis requiring immediate medical attention. Other signs may be present depending on the underlying cause (e.g. postural reaction deficits with polyneuropathy; regurgitation with concurrent megaoesophagus; coughing, pyrexia and malaise with aspiration pneumonia). Diagnosis: Complete blood cell count, biochemistry and thyroid profile should be performed. Thoracic radiographs are required to assess for megaoesophagus (10-20% of cases), aspiration pneumonia (7-15% of cases) and pulmonary odema. Various methods of diagnosing laryngeal paralysis include electromyography of the intrinsic laryngeal muscles to demonstrate denervation potentials, histopathology of these muscles to demonstrate denervation atrophy, or visualisation of the lack of abduction of the arytenoid cartilages and vocal folds through laryngoscopy (direct or video). More recently, diagnosis via ultrasound examination of the pharynx and larynx has been described. Laryngoscopy performed under a light plane of anaesthesia is by far the most commonly used diagnostic method in clinical practice. Traditionally thiopental was considered the drug of choice for laryngeal assessment however more studies have found alfaxalone, propofol, diazepam and ketamine are all suitable options. Any anaesthetic agent can obliterate normal laryngeal function even in healthy dogs. The key to diagnosing laryngeal paralysis is appropriate anaesthetic depth - a depth where the mouth can be opened for safe laryngoscopic assessment, but where the laryngeal swallow reflex is still present when the larynx is stimulated. Normally, the vocal folds and arytenoids are abducted on inspiration and passively relax on expiration. With laryngeal paralysis, the vocal fold(s) is/are immobile or may be paradoxically abducted on expiration - the assessor must be aware of the stage of the respiratory cycle during examination to avoid a false negative diagnosis with paradoxical movement. If arytenoid abduction is absent and excessive anaesthetic depth is suspected, doxapram hydrochloride can be used to stimulate deeper respiration.
Treatment: Medical treatment may be appropriate in cases that are only mildly affected. This involves weight loss, activity restriction and avoiding stress and heat. As most cases are progressive, owners should be warned that signs are likely to worsen with time and further treatment may be warranted. In animals with moderate or severe signs, surgery is recommended. Although several procedures have been described, unilateral arytenoid lateralisation (via cricoarytenoid or thyroarytenoid suture) or “laryngeal tie-back” is the most common. Unilateral cricoarytenoid lateralization involves placement of a nonabsorbable suture (typically 2-0 polypropelene) between the caudodorsal border of the cricoid cartilage and the muscular process of the arytenoid cartilage. Alternatively a thyroidarytenoid suture can be placed through the articular surface of the muscular process of the arytenoid and the caudodorsal border of the thyroid. Other procedures include bilateral arytenoid lateralization (not recommended due to unacceptable risk of aspiration), ventricular cordectomy and partial arytenoidectomy, transoral partial laryngectomy, modified castellated laryngofissure, and permanent tracheostomy. Animals that present in acute respiratory distress can often be stabilised medically with oxygen supplementation and light sedation (e.g. acepromazine 0.01-0.02mg/kg IV). Active cooling may be required. Prolonged upper airway obstruction may lead to pulmonary oedema requiring treatment with diuretics. If patients cannot be stabilised with medical therapy, emergency tracheostomy may be indicated. Complications and Prognosis: Clinical improvement is seen in approximately 90% of dogs undergoing unilateral arytenoid lateralisation and long-term prognosis is overall good. Complications occur in approximately 10- 60% of cases and include seroma, haematoma, aspiration pneumonia, persistent or recurrent coughing, persistent or recurrent inspiratory stridor and surgical failure from suture breakage or fragmentation of the arytenoid cartilage. Preoperative pneumonia, postoperative megaoesophagus and temporary tracheostomy have been significantly associated with postoperative complications and megaoesophagus has also been associated with increased risk of death. Aspiration pneumonia is reported in 8-21% of cases can occur years after surgery - dogs remain at risk of aspiration pneumonia for the rest of their lives. Feeding from a height is recommended ongoing to reduce this risk. Persistence or recurrence of strider and respiratory signs occurs in up to a third of dogs and is more common in small breeds.
| Tags:Most PopularVSS Resource Area |